CASE VIGNETTE – JANUARY 2020
Non Sequitur is a Real Phenomenon
It can often be accepted that an accident occurred. In addition, an injured party may exhibit significant impairment and loss. What is not always so clear is the presence or otherwise of a link between those two events.
The Latin term “non sequitur” refers to the truth incumbent in both statements, but the complete absence of causation.
I recently saw a 60 year old male who was a rear seated passenger in a motor vehicle which turned right across the path of oncoming traffic. His driver was obviously at fault but the injuries he sustained remained real.
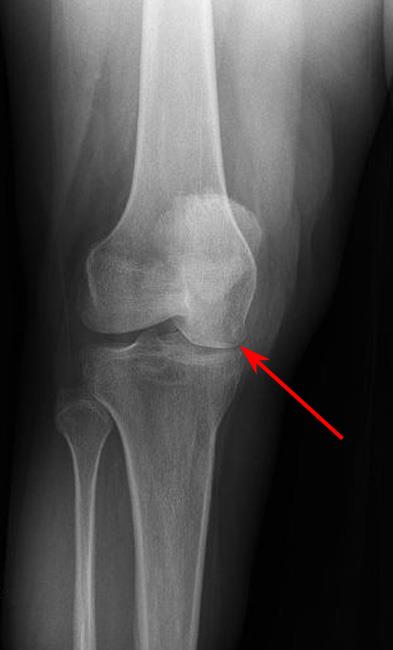
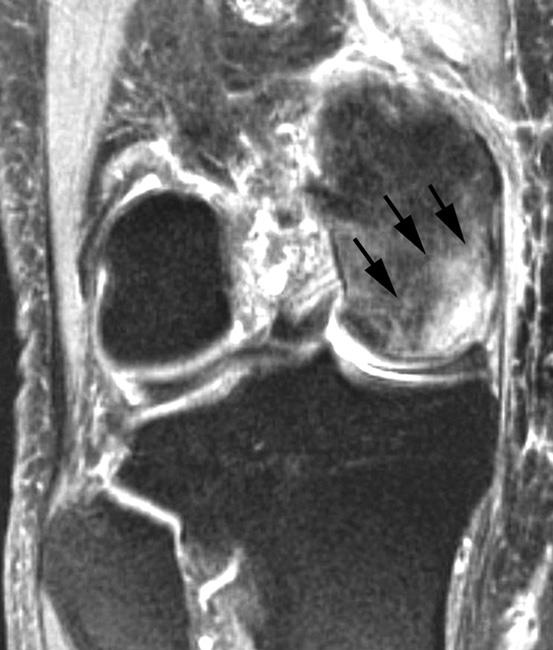
One of the injuries related to his right knee. There was a direct blow over the front of the patella (the knee cap) on the dashboard. This same knee had been subjected to an anterior cruciate ligament reconstruction 20 years previously. If the plaintiff was to be believed, the reconstruction had been an outstanding success and the knee joint had remained asymptomatic up until the time of this road traffic accident.
In assessing his circumstance, it appeared clear that whatever functional loss may have predated the accident as a result of the cruciate ligament reconstruction many years previously, it was not linked with the accident. Conversely, there was some additional loss that could be linked with the accident. The blow to the patella had damaged the joint between the knee cap and the high bone and had given rise to a measurable loss using the AMA 5 Guides.

Whilst the defendant’s team was keen to discount any knee problem as a result of the accident because of this positive past history, the plaintiff and his advisor were not easily dissuaded.
Common sense prevailed, compensation was forthcoming and to my mind, it was fair.
The lesson is important, and sometimes overlooked. Damaged goods can be made worse. A pre-existent functional impairment can be added to. Significant additional impediments can accrue.

It is only with a full history, a thorough clinical examination and a careful analysis that a true apportionment of blame can be identified.