
CASE VIGNETTE – JULY 2019
Not Everything Is As It Seems
Orthopaedic surgeons rely heavily upon radiographs to diagnose fractures. Fractures in themselves can be sub-classified in a myriad of ways. In essence however, a fracture refers to a discontinuity in the normal structure of a bone. Bones are living organs and have cortical and cancellous components.
Plane radiographs (and I use the word advisedly) are simply two-dimensional representations of a three-dimensional happening. Considerable overlay will be present on the film and an undisplaced, relatively minor fracture may not initially be visible.

The scaphoid bone (one of the small bones in the wrist) is a classic example. The scaphoid is about the size and shape of a cashew nut. It is vulnerable to fractures through the waist or the mid-section, especially in patients who sustain a fall on an outstretched hand or wrist.
The patient will almost invariably complain of pain in the so-called anatomical snuffbox (the small space just at the base of the thumb), but the initial x-ray or radiograph may show nothing untoward.
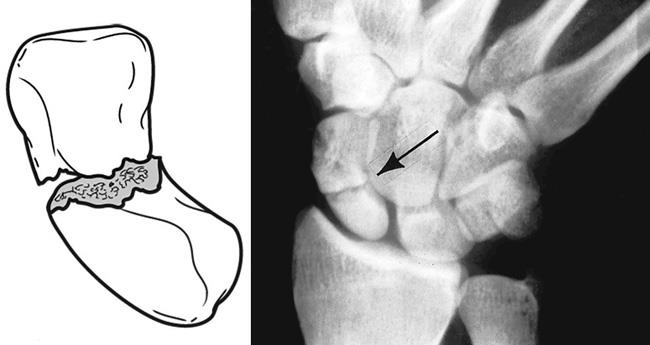
Part of the biology of fracture healing is initiated by so-called hyperaemia or an increase in blood flow with resorption of radio-opaque minerals at the fracture edges. Once this process has been in train for ten to fourteen days or so, some of the minerals are leached from the fracture zone and the region appears darker on a subsequent x-ray or radiograph. The diagnosis is then easier to make. As the healing process continues, new mineral is deposited, the area becomes more radio-opaque or white and the diagnosis is obvious.
The real trick here is to have a high index of clinical suspicion. If the patient does have a history of having fallen on an outstretched hand or wrist, does have considerable pain localised to the anatomical snuffbox and yet has a normal radiograph, it is prudent to immobilise the wrist as though a scaphoid fracture was present. The cast can then be removed two weeks later, a new radiograph performed and the underlying presence of a scaphoid fracture can either be confirmed or excluded.
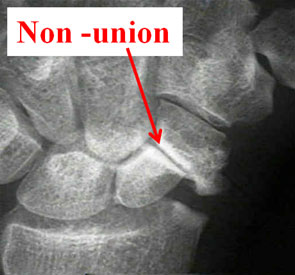
Failure to have this suspicion at the outset, and the failure to immobilise the wrist immediately, increase the risk of delayed or non-union with obvious ramifications.