
Case Vignette – June 2021
Scaphoid Fractures – Litigation Fodder
There are numerous small bones that form the wrist joint. They are divided into proximal and distal rows, with one of the bones partially crossing the divide. This is the scaphoid. It is shaped a little like a cashew and can be subject to injury with falls onto an outstretched hand. The injuries may be in the form of a ligamentous disruption within the wrist joint or alternatively, a fracture involving the scaphoid itself.
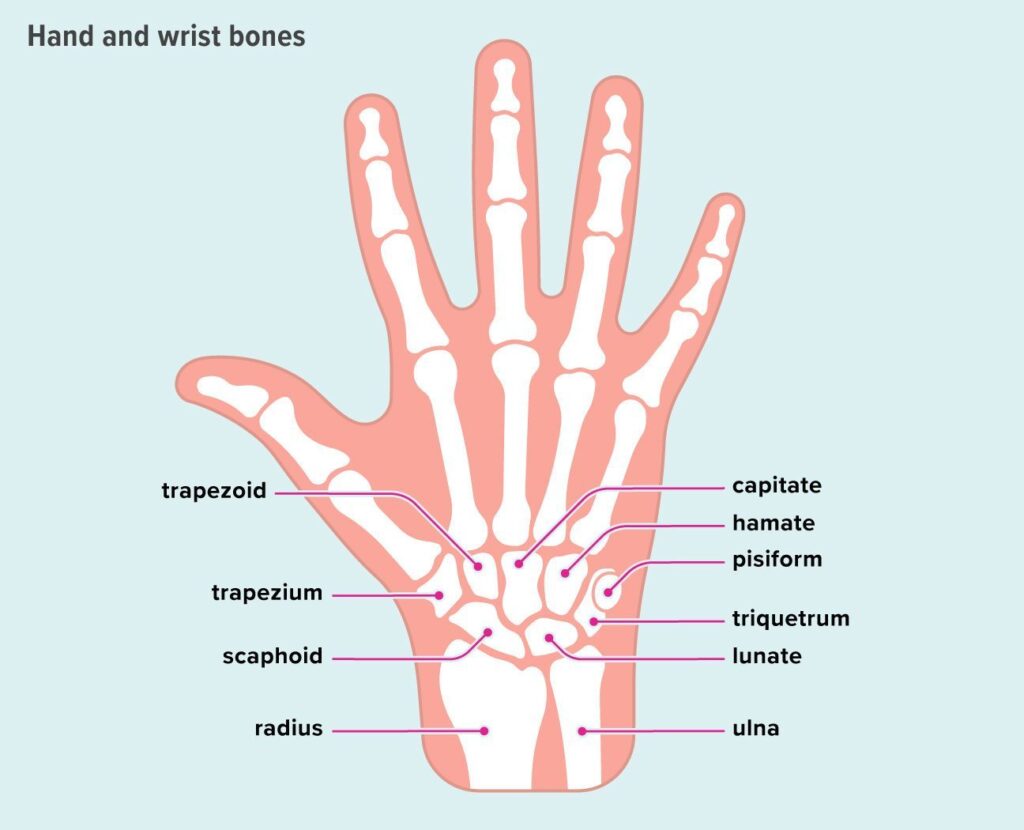
The scaphoid can be divided into thirds. The third closest to the shoulder is called the proximal third, whereas the third closest to the fingertips is called the distal third. Unsurprisingly, the remaining third is called the “middle third”!
Those fractures occurring in the distal third (the tuberosity) are usually of very little relevance.
The most common fractures do occur through the middle third (or the so-called waist) and can be subdivided into transverse, vertically oblique or horizontally oblique. They also usually unite although do require early and near-complete immobilisation in a special cast.

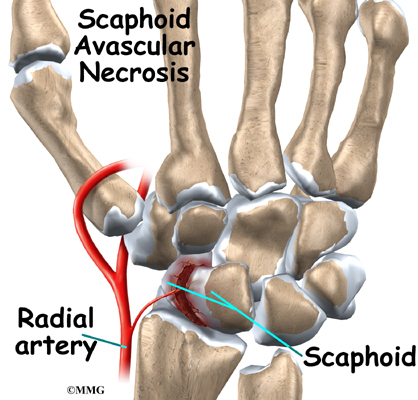
The fractures in the proximal third are a little more serious. They are subject to delayed union and avascular necrosis. Even non-unions can occur. Interestingly, even proximal fractures that do demonstrate avascular necrosis of the proximal third can go on to sound osseous healing.
The real issue here is that if the diagnosis is not made early and the scaphoid is not immobilised appropriately at that same time, delayed or non-unions can occur.
The typical patient would be a male who has had a motor cycle injury, presents to an Accident and Emergency Department for an x-ray, and is told that there is nothing to be seen. Over the next twelve months or so, he struggles on and re-presents with an established non-union and possible early osteoarthritis in the joint. The salvage is obviously far more difficult.
Proper care of a scaphoid fracture involves a high index of suspicion. Even if the original radiograph is normal, when a scaphoid fracture is suspected, the wrist should be immobilised and re-radiographed in 12-14 days. By then, the biological processes that follow a fracture will give rise to some so-called osteolysis (leaching of minerals) from around the fracture site and render it more visible on the subsequent x-ray.

Failure to have this index of suspicion and miss a scaphoid fracture may well be a basis for successful litigation.