
Case Vignette – July 2021
Osteoporosis of Pregnancy
Osteoporosis refers to demineralisation of the collagen structure in bone. It presents clinically as fractures caused by minimal force and radiographically by bones that are far less radio-dense than normal. Whilst the condition is often associated with age, and in particular in females, it can also rarely be associated with the third trimester of pregnancy in quite young women. Mothers at or about the age of 30 years appear to be particularly vulnerable and it is during the third trimester that hip pain (either unilateral or bilateral) is noted.

The diagnosis initially requires a high index of suspicion and this is not always present with all obstetricians. The diagnosis is best made with an MRI scan examination and the treatment modalities will differ according to the extent of the lesion that is identified.
Ideally, the condition is identified in its earliest phases, before a fracture of the femoral neck occurs and before anything more than rest and observation are required.

Sometimes, if the diagnosis is delayed, a fracture of the femoral neck may ensue. If that fracture is incomplete or undisplaced, it can be managed relatively easily with internal fixation. This is an orthopaedic endeavour that is not usually very difficult. Most fractures will then go on to sound osseous union with little or no long-term sequelae.
The most undesirable state however is when the diagnosis is delayed, a fracture occurs, the fracture becomes displaced and the risk of non-union, delayed union or avascular necrosis of the femoral head increases exponentially. If the fracture is displaced, many of these patients will eventually require a total hip replacement.
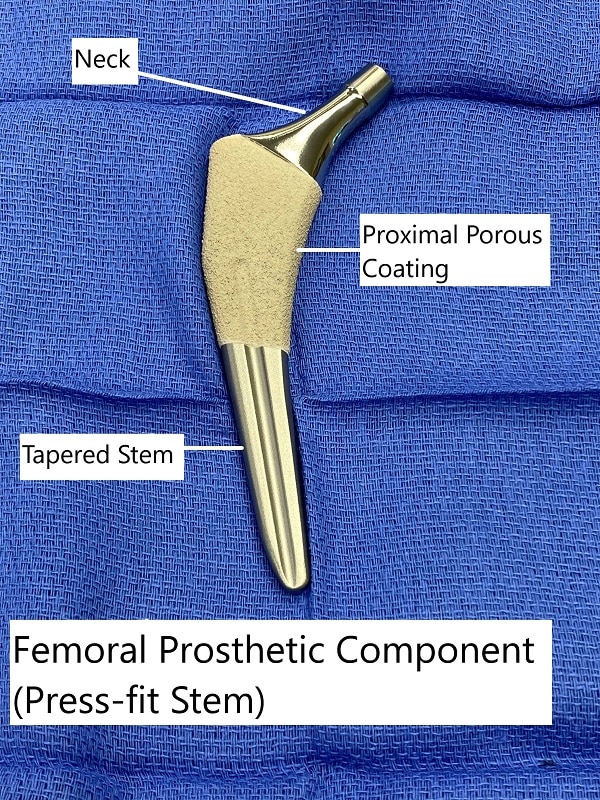
Whilst the hip replacement will solve the problem initially, it is an undesirable operative intervention in somebody who is in their early thirties. Hip replacements have a finite life span and theoretically, 10% of those patients will require a revision by the time they are in their early fifties. Of those, a further 20% will require a second revision in their seventies. Even a third revision may be required in the patient’s eighties, given actuarial longitudinal life studies that exist today.

It is important therefore that all clinicians involved in obstetric care have at least a high index of suspicion for this unusual and uncommon condition. Early diagnosis, proper orthopaedic care and judicious rehabilitation can effect an excellent outcome. If any or all of those elements are absent, the outcome can be far from desirable.