
CASE VIGNETTE – MAY 2020
Growth Plate Injuries and Their Importance
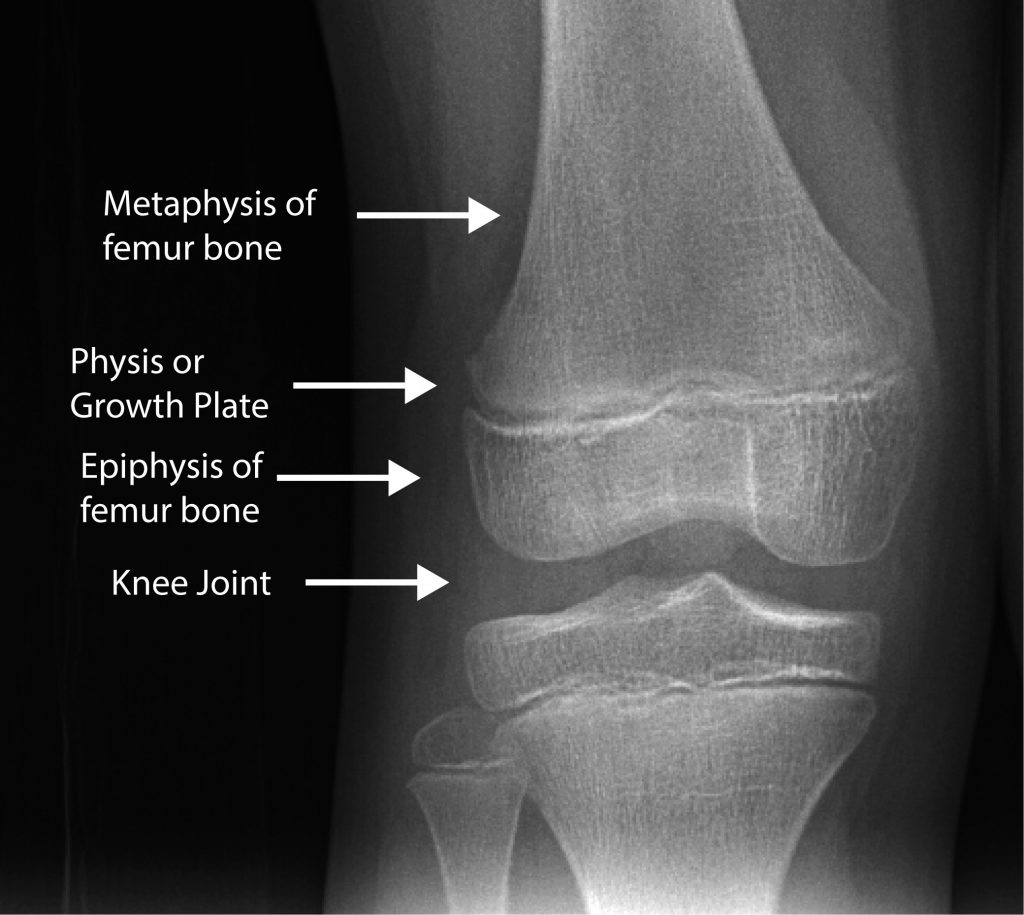
The long bones in our skeleton grow longitudinally. There are so-called growth plates at either end of the bone separating that part of the bone that forms a joint from that bone of the bone which forms the shank. The part that forms the joint is called an epiphysis and the part that forms the shank is called the metaphysis/diaphysis. The growth plate in between these structures is called the physis. The physis or growth plate is made up of cartilage in columns which grow incrementally with time. They continue growing until a person reaches so-called skeletal maturity. Longitudinal growth ceases, the cartilage ossifies (turns to bone) and the epiphysis is firmly united to the metaphysis/diaphysis. Further growth is impossible.
We refer to patients prior to closure of the physis as having an immature skeleton. This is in contrast to adults, who have a mature skeleton after the physes (physis plural) have closed.
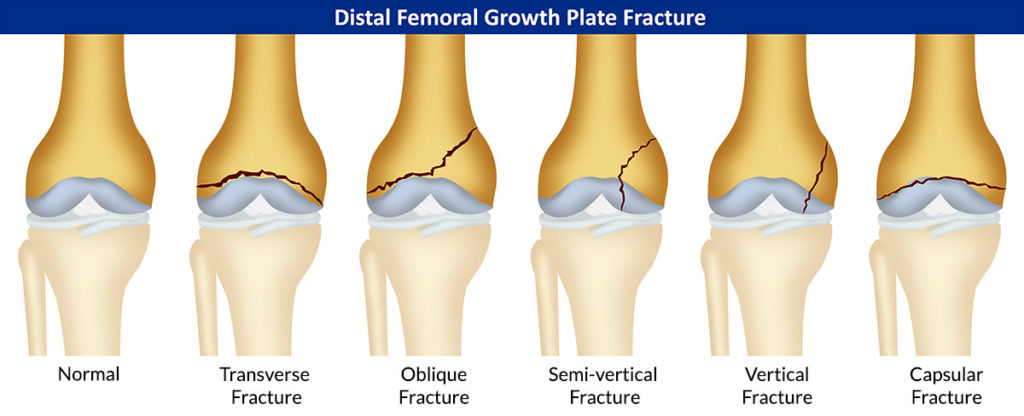
Fractures in long bones can occur not only through the bone (the epiphysis, the metaphysis or the diaphysis), but can also occur through the growth plate or physis. These physeal or growth plate injuries can be exceedingly sinister. There are five or six types described and the classification most commonly used was one described by Drs Salter and Harris from the Sick Children’s Hospital in Toronto.
The importance of these fractures lies in the risk of the cartilage plate healing partly or wholly with a bony or osseous bridge.
If the entire physis heals with bone, longitudinal growth is lost at that particular level. This can result in limb length inequality with shortening at that site. There are several measures at the disposal of an Orthopaedic Surgeon to manage this potential for limb length discrepancy before skeletal maturity occurs.
The other risk (and probably of greater importance) is when only part of the physis heals with the bony bridge whereas the remaining part continues to grow longitudinally. This circumstance will give rise to an angular deformity, which can be much more deleterious to the functioning of the neighbouring joint.
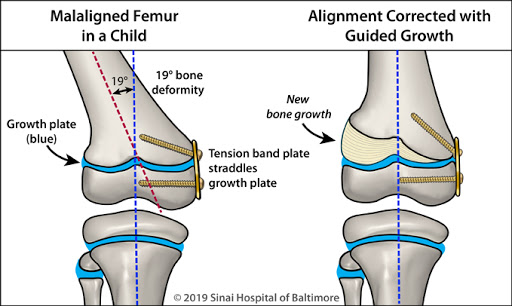
2 color figures showing the correction of a femoral deformity of the knee in a child. Figure 1 shows a tension band plate in the medial distal femur with a 19° deformity. Figure 2 shows the deformity corrected w guided growth.
It is imperative that physeal injuries are recognised early and managed properly by an appropriate specialist. If your client is a minor, and has sustained an injury of this nature, ensure that your expert is on top of the case. What might appear to be benign and of no great significance now, can assume much greater significance in the future as longitudinal growth proceeds.