
LEAD ARTICLE – FEBRUARY 2019
CLINICAL EXAMINATIONS AND SEXUAL BOUNDARIES
Whilst clinical examinations form a vital part of any orthopaedic assessment of a patient’s malady, examinations of an intimate nature are very rarely required. The definition of an intimate examination will vary from one observer to another but in general terms, it involves the clinical examination (both visual and manual) of the breasts and genitalia and may also include digital examination of the vagina or rectum.
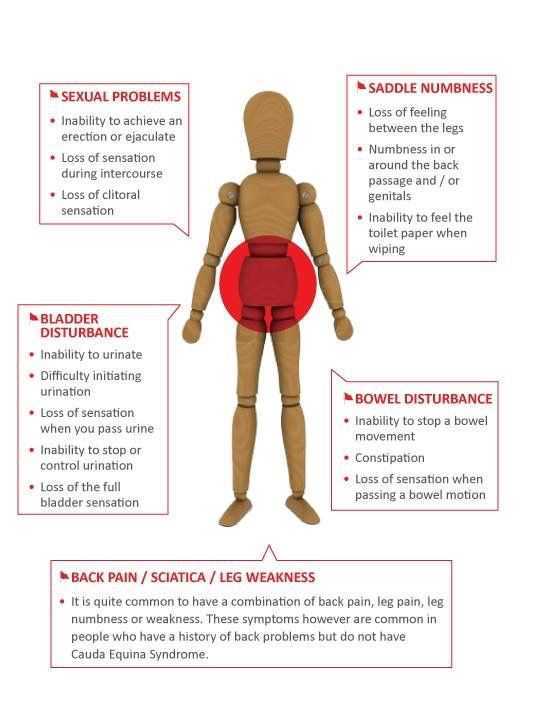
There will be some occasions when a rectal examination is important in an orthopaedic assessment. This will be to assess anal tone. Patients who suffer with cauda equina syndromes (where the lower nerve roots of the spinal cord are being compromised) can suffer with faecal and urinary incontinence and lack anal tone.
Neurological examinations of the lower limbs usually focus upon the exiting nerve roots from the spinal cord numbered L1 to S2. The genitalia are supplied by the nerve roots S2 to S4 inclusive. It is perfectly possible to thoroughly assess the neurological status of a lower limb without engaging in an intimate examination. If doubt should ever exist however, a chaperone should always be present. Most female patients would welcome such support. It should always be offered and whenever doubt exists, the presence of a chaperone should be insisted upon by the medical practitioner.
AHPRA, the Australian Medical Association and the medical defence organisations within Australia all publish guidelines and recommendations concerning these intimate examinations and the presence or otherwise of a chaperone or support person.

Patient dignity should remain paramount. Inappropriate comments, sexualised touching and activities that result in embarrassment are never acceptable.