
Case Vignette
Some Foot Injuries Are More Severe Than They First Appear
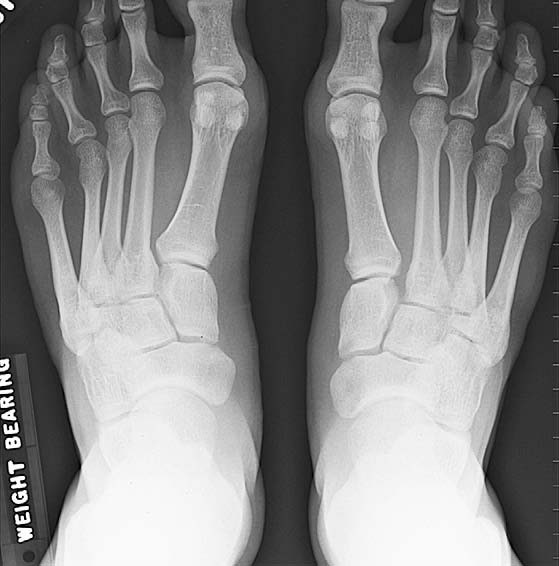
The foot is made of three components. There is the hindfoot with the calcaneus and the talus (the ankle bone), the midfoot with the tarsals and the bases of the metatarsals, and the forefoot with the metatarsals and the toes.
Hindfoot and forefoot injuries are usually quite obvious. Midfoot injuries however can be mistakenly overlooked. This combination of joints in the midfoot is sometimes known as the “Lisfranc” joint. The description refers loosely to the junction between the talus and the calcaneus behind and the cuneiforms and the cuboid in front. Those latter bones (the cuneiforms and the cuboid) also articulate with the bases of the first to fifth metatarsals inclusive.
This constellation of joints is of low range but does impart the ability for the midfoot to circumduct. The term refers to the ability to go upwards and downwards, inwards and outwards, and also rotate. The shoulder circumducts but obviously, the range of motion is vastly greater than the circumduction witnessed in the midfoot.

Twisting or crushing injuries can give rise to midfoot fractures and/or dislocations which can be quite difficult to detect clinically and with plane radiographs. Computerised scans are usually clearer and MRI scan examinations can also more accurately delineate the extent of the disruption. Technetium bone scans can also sometimes be of use.
Many midfoot injuries of the fracture/dislocation variety are missed. Healing takes place with the joints in deranged positions and with ligaments stretched, contracted or distorted.
The performance of the midfoot thereafter is permanently diminished. Patients will often present with stiffness, pain and midfoot swelling. They have difficulty wearing footwear, standing for prolonged periods, ascending or descending steps and slopes, and negotiating uneven terrain. If your plaintiff is a labourer, considerable remunerative losses may ensue.
From an expert opinion perspective, the AMA 5 Guides are not particularly useful. This injury is not described in specific terms. References are made to an increase or decrease in the height of the arch of the midfoot and allowances are also made for x-ray appearances consistent with post-traumatic osteoarthritis. It is possible however that your plaintiff may have quite severe symptoms, marked limitations in ambulatory capacity and a severe interruption in his or her lifestyle without those obvious features. Chapter 17 of the AMA 5 Guides may yield very little in the way of functional impairment. The disability however can be quite large. It is imperative that your expert understands these concepts and explains them in detail in the absence of your prompting. Whilst you may be excellent with the legal intricacies of your plaintiff’s case, you cannot always be expected to know the precise questions which will elicit the appropriate responses from your expert. Choose wisely.