
Case Vignette
Do All Shoulder Injuries Require Surgical Intervention?

No.
Many patients over the age of 40 years already have some intrinsic degenerative change within the soft tissue restraining structures around the shoulder joints. Those restraining structures are collectively known as the rotator cuff and are formed by a condensation of tendons passing between muscles in the shoulder joint and the upper end of the arm bone, and the surrounding capsule itself. The degenerative change is obviously age-related but can be due to a variety of activities of a social, recreational, domestic or remunerative nature. Some patients are more susceptible than others and some patients, although exhibiting MRI scan examination features of degeneration, can remain completely asymptomatic indefinitely. Some patients, from that asymptomatic group, may even have partial or full thickness tears of a partial or complete nature.
When an injury is superimposed upon these underlying pre-existent asymptomatic pathological tissues, a symptom complex can become manifest. Typically, patients will note the sudden onset of discomfort with a provocative manoeuvre and will thereafter be plagued by pain, weakness and often quite a significant restriction in range of motion.
Can Treatment Interfere with Litigation?

Almost all of those patients should be managed non-operatively initially. Over a six months period or thereabouts, many patients will improve considerably and may even return to the pre-accident asymptomatic state despite the persistence of the underlying pathology. Some patients may suffer with so-called frozen shoulder during that six months period. The true cause of frozen shoulder or adhesive capsulitis is elusive. It is characterised by increasing pain and a concomitant reduction in movement. The pain typically reaches its zenith and the range of motion diminishes to almost nothing. That situation prevails in a so-called plateau period for months and then, the whole process gradually reverses. That is to say, the pain gradually diminishes, the range of motion improves and many patients will return to complete symptomatic normality. The whole process may take as long as eighteen months. Considerable debate exists about the wisdom or otherwise of performing any operative procedure during that period. There are some surgeons who say the frozen shoulder should be left well alone until nature handles the matter herself. Others believes that operative intervention can be of some assistance.
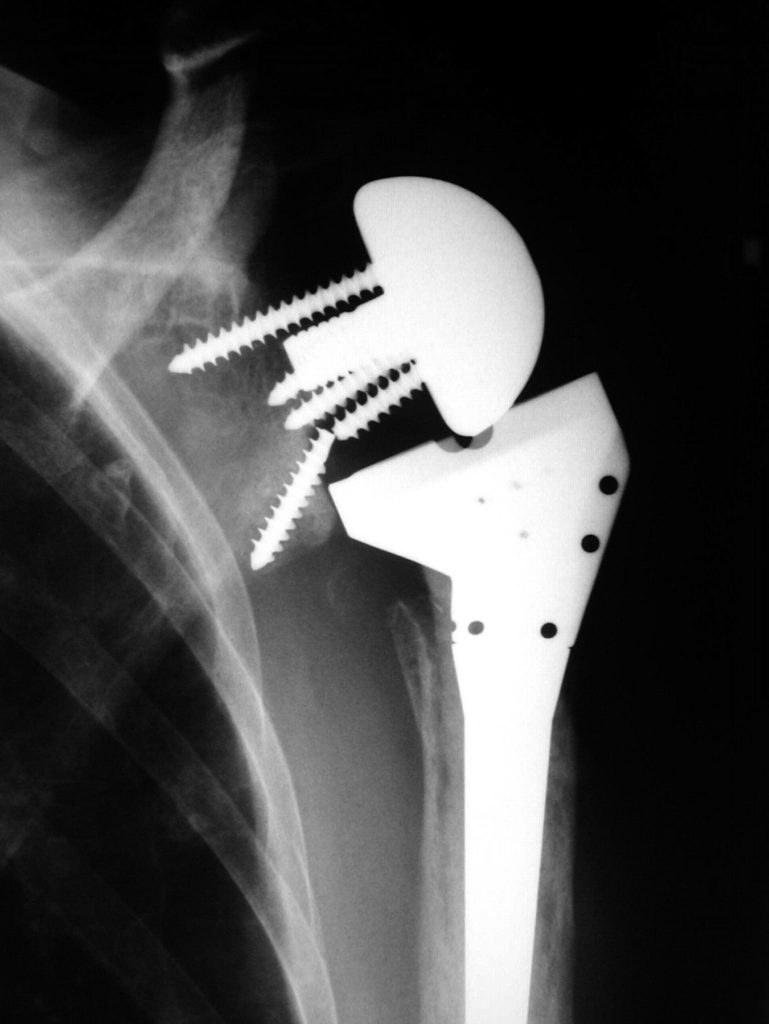
Whatever the true answer, premature operative intervention can definitely make things worse. Failed surgery may lead to revision surgery. Some patients may even undergo a third form of reconstruction. A subset of that group may even be subjected to a so-called reverse shoulder joint replacement.
When an observer casts his or her mind back to the original injury, and the natural history of that injury, some pity must be had for the patient who has followed that course of multiple operations. In all probability, that patient would have been better left well alone.
Who Should Pay?
The question then occurs – who should be responsible for the final circumstance after that undesirable sequence of events? Should it be the original defendant or should the unwise orthopaedic surgeon take some of the blame? Whilst from a theoretical standpoint, both groups have contributed in some way together, in practice: differentiating between the two can be very difficult. In my experience, it is usually the first defendant who carries the blame. I often wonder if this is fair?